As we have all heard there are many myths in ophthalmology. Some of these myths are” things” our patients believe and therefore reiterate. Then there are myths that many of us ophthalmologists believe often without good reason or proof. Perhaps because a respected mentor told us that many years ago. I have asked several ophthalmic friends for their input concerning various ophthalmic misunderstandings/misconceptions. Their names will remain anonymous to protect the misinformed / the innocence. This has been a fun project for me and several friends have enthusiastically contributed. If any of you can name other myths especially myths we ophthalmologists believe, I would like to hear from you.
First are several myths that I have tried over the years to debulk — unsuccessfully.
- Phenylephrine ( Neo-Synephrine ) 10% is somehow dangerous —-> hypertension, tachycardia , etc. ? I have used 10% for years with no adverse effects although I have not checked routinely the pulse / BP of these patients. I would not recommend using in children under age say 10 years. Some people believe little additional mydriasis response is achieved by increasing the strength above 5%. This could easily be a residency study — comparing systemic side effects of 10% phenylephrine with 2 1/2%, and controls ( just tropicamide ? ).
- Our patients should not “bend over” post-op cataract extraction and should not sleep on the operative side. Really? Do not lean over to put on your shoes, do not lean over to make up your bed, put something in the oven, etc. Years ago I did a Medline search concerning sleeping on the operated side and could find no adverse cases from sleeping on the side of the eye operation. We might want to tell post-op patients not to rub the eye/eyelids and not to pick up anything weighing more than say, 20 lbs although even that might be suspect/incorrect.
- Myths From the Patient’s Standpoint ( lots of responses here ) :
- A child will often ”outgrow” their strabismus —-( pseudostrabismus from prominent epicanthal folds ? )
- Wearing glasses will make the eyes worst.
- Too much reading / close work causes myopia. Probably true.
- Computers will damage your vision if used too long. Dubious.
- Watching too much TV makes the eyes worst. Well, probably not the eyes.
- “Colorblindness “ in a male means he can’t see any color at all. Not exactly.
- Sitting close to the TV means the child needs glasses / “something’s wrong”.
- Reading in low or poor lighting will ruin/harm your eyes.
- Carrots help vision. Well, perhaps true with xerophthalmia ( beta carotene ).
- Don’t fly commercially after cataract surgery.
- Eye exercises will help vision/reading ability. If “junior” isn’t reading at age 7 and in a middle-class educated family, bad things could happen to that young child pediatric neurologist, pediatric psychologist, imagining, social workers, occupational therapists, “eye training exercises”, etc. Actually vision therapy/exercises do not “help“ autism nor poor reading skills, etc. Often a useful way of doing a wallet – ectomy on the parents. Some kids esp. boys are just not ready to read until a little later ( ? 8 or 9 years ). As the child gets older his reading skills might improve simply with time (aging) and all the positive feedback ( encouragement ).
- With dilation, need to keep the eyes shut and the lights off.
- Paraorbital headaches mean a brain tumor. Unlikely but possible.
- Cataracts are on the surface of the eye and can be scraped or peeled off. Changing my glasses will make me see better even if I have cataracts.
- If you cross your eyes as a child, your eyes will stay that way.
- Cataracts need to be ripe before they can / should be removed.
- When you do a corneal transplant, you take the whole eye out, put it on the cheek, fix it, and then put it back in the orbit.
- “I’m not losing my ability to focus close up and it isn’t due to aging. You should be able to fix this ( presbyopia ). If I had never gotten that first pair of reading glasses ( “ cheaters” ), then I would not need reading glasses now”.
- Loss of some vision in one eye, means I qualify for disability.
- “Those drops do not work with my glaucoma, my vision is still not good.” And yes the second leading cause of blindness worldwide is glaucoma.
- You can transplant the whole eye.
- I get all my eye care information from “ Dr. Google.” However, Dr. Google is not always correct.
- Myths from the ophthalmic community – this was most surprising to me
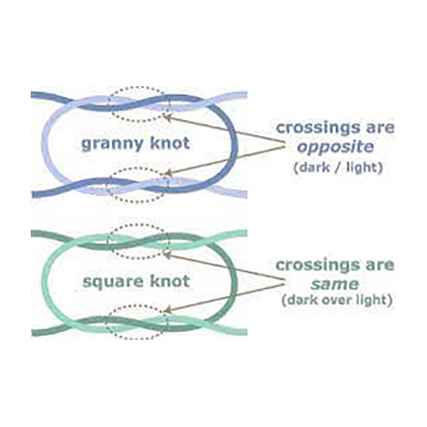
- “Granny knots are bad”. Actually, it doesn’t matter— granny and square knots are both OK. No difference in knot / tensile strength. Think of all the poor eye residents that have been merciless berated for years without cause.
- Some patients with corneo-scleral lacerations can do well. I have never seen any patient with an ocular laceration involving the ciliary body retain any useful vision. The eye slowly heads toward phthisis.
- If I prescribe the drops, then the drops will somehow “work better” than if another eye doctor prescribes the same drops. Good luck with that thinking.
- “We tell all our glaucoma patients to wait 5 -10 minutes between each drop”. I used to see “ new “ glaucoma patients who had retired to low country S.C. from elsewhere who were using their drops right on top of each other. According to the patient, “no one ever told me that before.” I think it is likely our patients were initially told that but somehow forgot those instructions. This is not uncommon if you see “new“ patients already on topical glaucoma drops. When I have mentioned this to other ophthalmologists, the response is “ we always tell our patients to wait 5 minutes”. Possibility the patients were initially told that, but have forgotten those instructions. When you tell the patient they are not getting the full effect ( dilution ) of either drop, then the “ light bulb “ often comes on. This is often true with ophthalmic suspensions. If you don’t shake ( 40 times ), you are not getting the full affect. Sometimes on the bottle , it even says “ shake well”. But the patient is not “ shaking well “ This is certainly true for Pred Forte, Azopt, etc.
- “Expired drops are bad”. WelI , from a medicolegal standpoint, I would certainly not use any expired drops in North America. However, I have used many expired drops for many years in many different countries ( low-income / middle-income ). I have never seen any adverse affects . An expired drop ( bottle ) does not magically turn into sulfuric acid or other caustic solution immediately after the expiration date. Perhaps after 3 – 5 years the expired drops are not as effective but 80 % effective for say Vigamox is much better than nothing. Right?