I wanted to write again on glaucoma as we all see many patients with glaucoma everywhere — many unfortunately with severe, advanced, end-stage glaucoma when we first see them. As you know, glaucoma is the second leading cause of blindness in the world after unoperated cataracts. Most of what I will say, I’m sure you have heard previously.
Glaucoma can be a difficult disease to diagnosis and treat / maintain. End stage glaucoma is unfortunately often easy to diagnosis as the patient may have marked visual field constriction as well as poor vision OU. You can often rather easily make the diagnosis of end-stage glaucoma as the glaucoma patient can not locate / find ( ambulate ) the eye chair or does not see your extended hand to shake due to the markedly constricted visual fields.
There is no magic number to determine normal patients without glaucoma from patients with glaucoma. You can not say everyone with an IOP over 23 mm has glaucoma and needs treatment for the rest of their life and everyone under 23mm is OK without glaucoma. Life would be easier for the eye health worker if that was true. Please don’t chase / treat the number. Please check IOP a lot ( record ).
However, usually the higher the IOP the more likely that the patient does indeed have glaucoma. Patients can have ocular hypertension with IOP over 22 mm but normal optic disc ( c/d ratio ) and normal visual fields / OCT ( RNFL ). Those patients probably do not have glaucoma and do not need treatment. They certainly need to be followed closely and have frequent IOP checks.
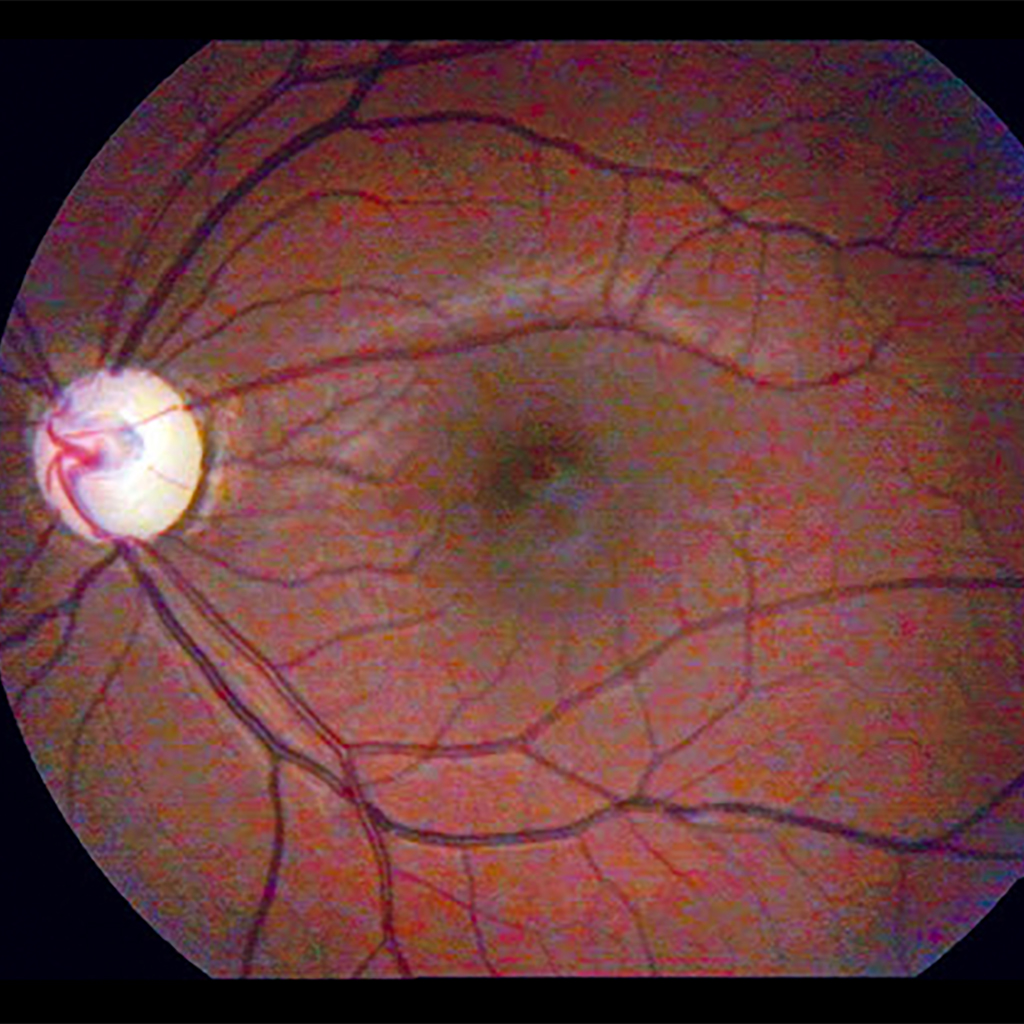
Then there are patients that have normal tension glaucoma with IOP’s never above 21 mm but do indeed have glaucoma and need treatment — abnormal c/d ratio ( enlarged ) and abnormal visual fields / OCT. Glaucoma, early on, is not an easy disease to diagnosis and possibility treat or not treat.
OCT ( RNFL / retinal nerve fiber layer ) is often useful in helping to rule in or rule out early glaucoma. I would not refer glaucoma patients with severe advanced glaucoma for OCT because you already know the nerve fiber layer is thin and you will see a lot of red in the results. No use having the patient and family travel to Belize City for OCT at additional cost for patient and family. No useful information, as you already know the patient has severe glaucoma.
Visual fields ( perimeter ) are quite useful with glaucoma but the patient needs to be taught how to take test. Often the first visual field results are not reliable.
I have left several reference books at all of our clinics: #1. The Physicians Guide to Eye Care #2. Practical Ophthalmology ( blue cover ) #3. Basic Ophthalmology #4. Eye Care in Developing Nations by Dr. Larry Schwab who has spent many years in low-income and middle-income countries. Please read these books and use them as references. Almost every eye problem you will see is described in one or more of these great books.
We can not rule in ( diagnosis ) glaucoma with just the IOP reading. We now have three portable glaucoma measuring devices ( tonometers ) scattered about the country [ I-Care, 2 and TonoPen,1 ]. They can be quite useful in our clinics ( speed up examinations ) and with our outreach activities. Big help. But again you can not use just the IOP to diagnosis as you will be wrong a lot of the time ( ocular hypertension / normal tension glaucoma ). This is why only checking the IOP is not used as a screening technique to diagnosis glaucoma.
Laser trabeculoplasty is not an emergency procedure. Laser trabeculoplasty will not cure glaucoma nor restore vision. However it sometimes reduces the IOP but usually the patient will usually still need to be on treatment ( drops ). You should tell patients that the laser treatment will not improve their vision.
Most of our patients will need to be on more that one glaucoma drop ( agent ) to control their IOP. Timolol is usually effective, cheap, and usually readily available. However often the patient needs more that just timolol to reduce the IOP significantly. That is why some of our glaucoma medicines are actually combinations. You should have your patient bring their drops to their follow up appointments. If you do that, you will be surprised how often your patients are using the drops incorrectly.
Adherence / compliance ( using any medicine as prescribed ) is quite poor with glaucoma. Many of our patients can simply not afford their drops.
Patients with severe optic nerve damage need their IOP as low as possible to prevent further progression ( damage ). Below 15 mm is ideal but often difficult to achieve.
Please give out the glaucoma handouts so our patients can learn more about their disease.
Please ask glaucoma patients to have their family members checked for glaucoma every two years.
Thanks for your efforts.
Peace, Baxter